I decided a little while ago that I'm not going to try to include a coronavirus chapter in the book. It would have been possible if I wanted to. I really used three methods to find artifacts -- searching in as many candidate museums' online catalogs as were available, emailing people at museums directly, and asking around (usually with the goal of finding more places to search or email). For this one, I would have started by asking around. I know that a lot of museums are actively collecting pieces of culture from this crisis. (Here's a list!) When museums, especially history museums, collect items from the present day, it's often called "rapid response collecting," and I talk about this a bit in my chapter on Narcan, the opioid overdose antidote. Many museums are asking people to contact them about donations but not to send them to the museum yet, as many museums are still fully or partially closed. But, all I would need is confirmation that the museum plans to accession a particular item (meaning formally making it part of their collection), a photo, and a bit of the item's story.
I'm not doing that. (Okay, I won't promise that, my editor could still persuade me otherwise, for example). I don't think there's a perfect answer to whether it should be in the book or not, but I'll share my thought process here. The book will be about 50 artifacts, no more, no fewer, but I do have some chapters I could do without if I needed to make room, not because they're not good, but because they are less central to the book's theme than others. Part of it is just for my own time management. I mentioned my decision to some friends, and several of them had published books or articles relevant to a developing story. One had a book that was largely about national politics and it was in proofs (the last stage of editing, after everything has been laid out) when Trump was impeached. Sometimes, you have to come up with a cut-off for what a piece will cover, or it will never go to print.
Obviously, it's too soon to say what the historical meaning of coronavirus will be, even though plenty can be said about its present impact. In a few other chapters about recent or recent-and-ongoing history, I put a modern artifact in its historical context and explain how we got here. The chapter centered around an ambulance in the events of September 11, 2002 is a chapter about the history of emergency medical services, and the chapter centered around Narcan is about the past and present of opioid use, misuse, and treatment. So, I could put coronavirus in context by talking about the history of pandemics, quarantine, and social distancing, or the modern technologies that enabled science to identify specific viruses. Part of the reason I don't plan to, though, is that a lot of other writers are putting the virus in its historical context right now. I believe that the people who are likely to read my book will have a pretty high overlap with the people who will have been reading about coronavirus in its historical context for a year by the time it comes out. Several years from now, when there are readers for my book who were too young to have been keeping up with the news in 2020, those readers will also have access to information about coronavirus written with the benefit of hindsight.
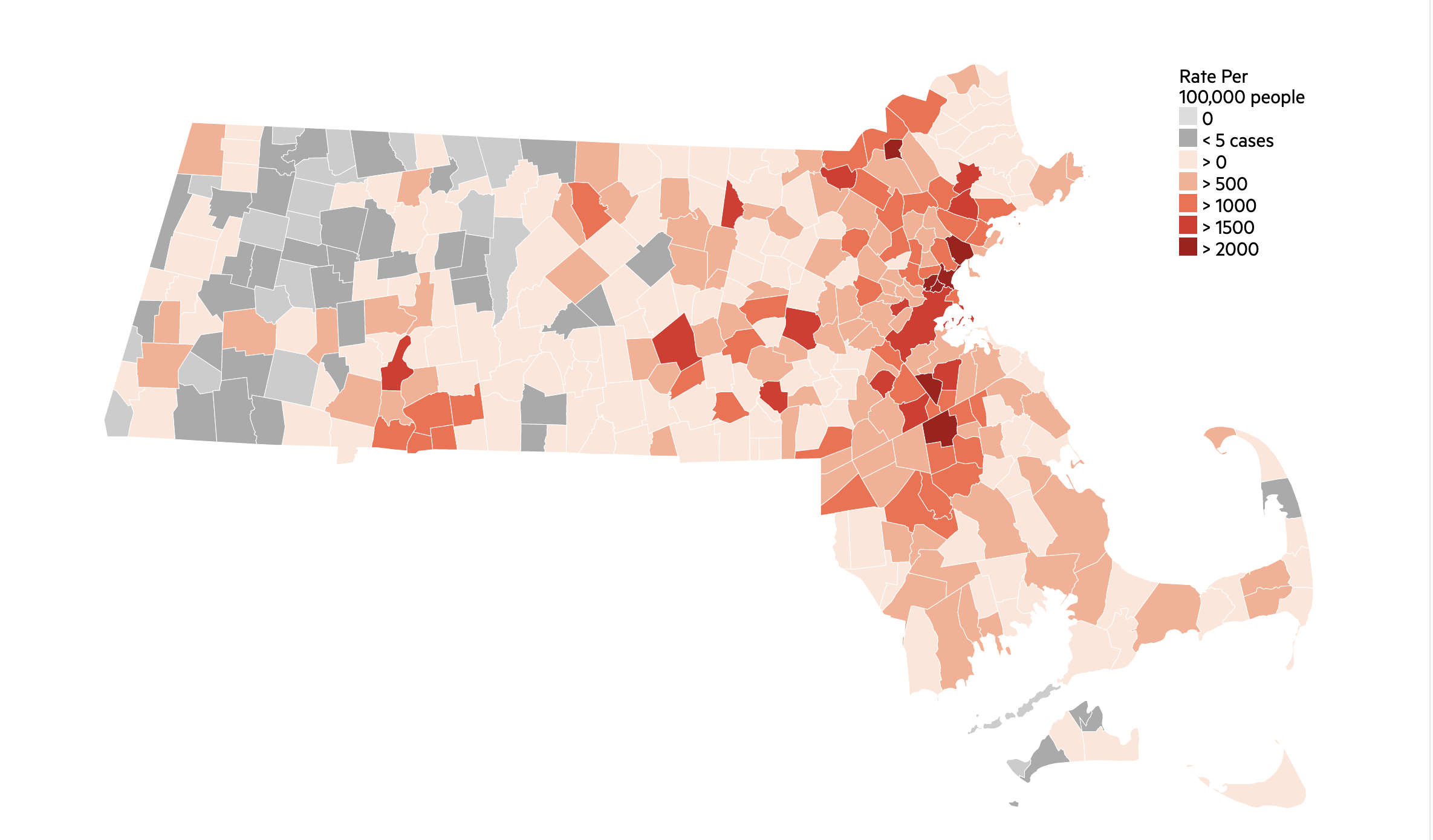
Distribution of rates of coronavirus cases in Massachusetts. Data from the Massachusetts Department of Health, infographic from https://www.wbur.org/commonhealth/2020/03/09/coronavirus-cases-massachusetts-map
If I did write this chapter, it would be a challenge for me not to make it about health and healthcare disparities -- or a challenge to do so, but to do it well in a short chapter. Frankly, I'm much more comfortable writing about historical disparities with an eye to the ways they continue today than tackling current disparities. I know there are others more others more comfortable and equipped to write about the present day. Thankfully, we don't all have to do it all. The book does have introductions to the history of American health insurance, pseudo-scientific attitudes towards race,, and Black people organizing for better healthcare in the early 20th century, and it frequently mentions the way poverty and working conditions affect health -- I am a social historian at heart. It's just... I could spend a whole chapter expressing rage at the fact that Chelsea, MA has seen 2,928 cases of coronavirus to date (in a city of just over 40,000 people), while my town of Arlington, nine miles away, has seen 305 cases (in a town of not quite 43,000).
One final reason, although I can see both sides to this one even more so than the other reasons, is that I expect many people to be coronavirused-out by the time the book comes out. They could skip that chapter, sure, but I'd rather give people a book they want to read all of. The flip side is that while coronavirus will be real, painful, and current or recent to most-to-all readers, there are other chapters that will be real, painful, and current to some readers anyway. I've already mentioned the opioid crisis chapter, the AIDS crisis is only over if you have good and consistent access to expensive healthcare, and tuberculosis is still a major killer around the world and in prisons and on Native reservations.
None of this is particularly to defend my choice not to include that chapter. In some ways it's a more vulnerable and more negative blog post than I usually write, but my hope is that it gives you a further peek into what's on my mind while juggling the book and living in 2020.
Sources on infection numbers:
https://www.chelseama.gov/coronavirusupdates
https://www.arlingtonma.gov/departments/health-human-services/health-department/coronavirus-information
I'm not doing that. (Okay, I won't promise that, my editor could still persuade me otherwise, for example). I don't think there's a perfect answer to whether it should be in the book or not, but I'll share my thought process here. The book will be about 50 artifacts, no more, no fewer, but I do have some chapters I could do without if I needed to make room, not because they're not good, but because they are less central to the book's theme than others. Part of it is just for my own time management. I mentioned my decision to some friends, and several of them had published books or articles relevant to a developing story. One had a book that was largely about national politics and it was in proofs (the last stage of editing, after everything has been laid out) when Trump was impeached. Sometimes, you have to come up with a cut-off for what a piece will cover, or it will never go to print.
Obviously, it's too soon to say what the historical meaning of coronavirus will be, even though plenty can be said about its present impact. In a few other chapters about recent or recent-and-ongoing history, I put a modern artifact in its historical context and explain how we got here. The chapter centered around an ambulance in the events of September 11, 2002 is a chapter about the history of emergency medical services, and the chapter centered around Narcan is about the past and present of opioid use, misuse, and treatment. So, I could put coronavirus in context by talking about the history of pandemics, quarantine, and social distancing, or the modern technologies that enabled science to identify specific viruses. Part of the reason I don't plan to, though, is that a lot of other writers are putting the virus in its historical context right now. I believe that the people who are likely to read my book will have a pretty high overlap with the people who will have been reading about coronavirus in its historical context for a year by the time it comes out. Several years from now, when there are readers for my book who were too young to have been keeping up with the news in 2020, those readers will also have access to information about coronavirus written with the benefit of hindsight.
Distribution of rates of coronavirus cases in Massachusetts. Data from the Massachusetts Department of Health, infographic from https://www.wbur.org/commonhealth/2020/03/09/coronavirus-cases-massachusetts-map
If I did write this chapter, it would be a challenge for me not to make it about health and healthcare disparities -- or a challenge to do so, but to do it well in a short chapter. Frankly, I'm much more comfortable writing about historical disparities with an eye to the ways they continue today than tackling current disparities. I know there are others more others more comfortable and equipped to write about the present day. Thankfully, we don't all have to do it all. The book does have introductions to the history of American health insurance, pseudo-scientific attitudes towards race,, and Black people organizing for better healthcare in the early 20th century, and it frequently mentions the way poverty and working conditions affect health -- I am a social historian at heart. It's just... I could spend a whole chapter expressing rage at the fact that Chelsea, MA has seen 2,928 cases of coronavirus to date (in a city of just over 40,000 people), while my town of Arlington, nine miles away, has seen 305 cases (in a town of not quite 43,000).
One final reason, although I can see both sides to this one even more so than the other reasons, is that I expect many people to be coronavirused-out by the time the book comes out. They could skip that chapter, sure, but I'd rather give people a book they want to read all of. The flip side is that while coronavirus will be real, painful, and current or recent to most-to-all readers, there are other chapters that will be real, painful, and current to some readers anyway. I've already mentioned the opioid crisis chapter, the AIDS crisis is only over if you have good and consistent access to expensive healthcare, and tuberculosis is still a major killer around the world and in prisons and on Native reservations.
None of this is particularly to defend my choice not to include that chapter. In some ways it's a more vulnerable and more negative blog post than I usually write, but my hope is that it gives you a further peek into what's on my mind while juggling the book and living in 2020.
Sources on infection numbers:
https://www.chelseama.gov/coronavirusupdates
https://www.arlingtonma.gov/departments/health-human-services/health-department/coronavirus-information
x
Comments
Post a Comment